Insomnia Treatment in Austin
When trying harder to sleep becomes part of the problem
I provide CBT-I (Cognitive Behavioral Therapy for Insomnia), the first-line, evidence-based treatment for chronic insomnia for adults in Austin and throughout Texas via telehealth.

Jessica Fink, LCSW-S offers CBT-I in Austin and across Texas via telehealth
If you've struggled with insomnia for any length of time, you've worked tremendously hard to fix the problem.
Sleeping in later.
Taking melatonin.
Cutting out caffeine.
Meditation.
White noise.
Sleep hygiene.
Maybe some of those things helped a little. Maybe nothing improved at all.
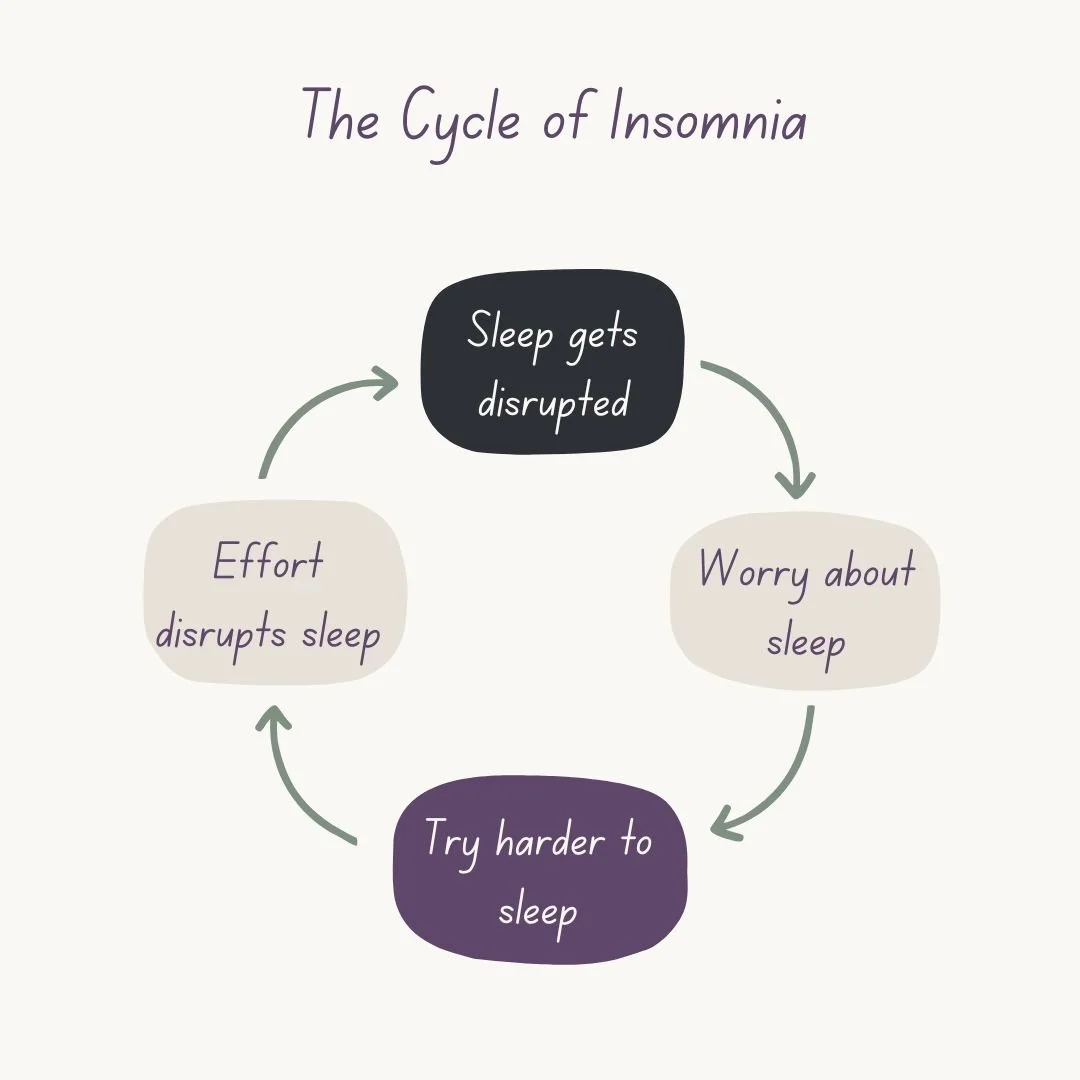
Or, most annoyingly, maybe as you kept trying harder and harder, the problem got worse.
If you're feeling frustrated and out of options, I'd like to validate something I'm sure you've already noticed.
Sleep does not reward effort. At all.
Most people with chronic insomnia are working harder than anyone they know to get sleep. They think about sleep all the time, they're doing everything they were told to do, and their sleep hygiene is top-notch. Meanwhile, they can't help but notice that the good sleepers in their life are doing nothing right and sleeping beautifully.
You know how, for most problems in life, you overcome them by setting a goal, working hard, and not giving up until you achieve it?
Throw all that out the window.
Sleep plays by a completely different set of rules.
What is Insomnia?
Most people think insomnia simply means not sleeping.
There's more to this problem than that.
Everyone has bad nights from time to time. Insomnia is a recurring problem that takes over your life.
You might have difficulty falling asleep, staying asleep, or both. Despite being labeled a sleep disorder, it's really a 24-hour issue because it affects your days just as much as your nights.
And here's something many people aren't aware of.
Difficulty falling asleep doesn't automatically mean insomnia.
Sometimes it's insomnia.
Sometimes it's a delayed body clock.
Sometimes it's both.
That's why understanding the problem comes before choosing the treatment.
Why Does Insomnia Keep Going?
People often assume insomnia means their body has forgotten how to sleep. Fortunately, that's usually not what's happening.
Sleep is an automatic biological process.
Breathing.
Digesting food.
Sweating.
Falling asleep.
These are all things your body knows how to do without conscious effort.
In fact, trying to voluntarily control an automatic process usually makes it harder, not easier.
Have you ever been doing something you've done a hundred times, noticed someone was watching you, and suddenly forgotten how to do it?
It's not that you lost the ability.
You became so aware of what you were doing that it got in the way of doing it.
Sleep is a lot like that.
Another problem is that our brains are really good at making associations.
Have enough bad nights, and your bed can gradually become associated with:
frustration,
alertness,
worrying,
clock-watching,
trying to force sleep,
wondering how you'll function tomorrow.
Instead of becoming a cue for sleep, your bed gradually becomes a cue for wakefulness.
That isn't something you chose. It's something your brain learned. And what is learned can also be unlearned.
Why Trying Harder Usually Doesn’t Work
One of the most frustrating things about insomnia is that the things people naturally do to solve it usually make perfect sense.
Going to bed earlier
Sleeping in
Lying in bed hoping sleep will eventually come
Canceling plans because you're exhausted
Watching the clock
Trying harder to fall asleep
None of these behaviors seem wrong. They’re problem-solving behaviors.
Unfortunately, many of them unintentionally keep the insomnia going.
That's one of the reasons Cognitive Behavioral Therapy for Insomnia (CBT-I) is so effective.
Instead of asking:
"How do we make you sleep tonight?"
We're asking:
"What is keeping your brain from sleeping the way it naturally knows how?"
What Is CBT-I?
Cognitive Behavioral Therapy for Insomnia (CBT-I) is considered the first-line treatment for chronic insomnia by organizations including the American Academy of Sleep Medicine and the American College of Physicians.
CBT-I works by identifying and changing the conditions that keep insomnia going.
Treatment may include:
rebuilding the connection between bed and sleep,
adjusting time in bed to strengthen your natural sleep drive,
developing a more consistent sleep schedule,
addressing unhelpful beliefs about sleep,
reducing the cycle of frustration that often develops around bedtime.
Every recommendation has a purpose. I'll explain not only what we're doing, but why we're doing it.
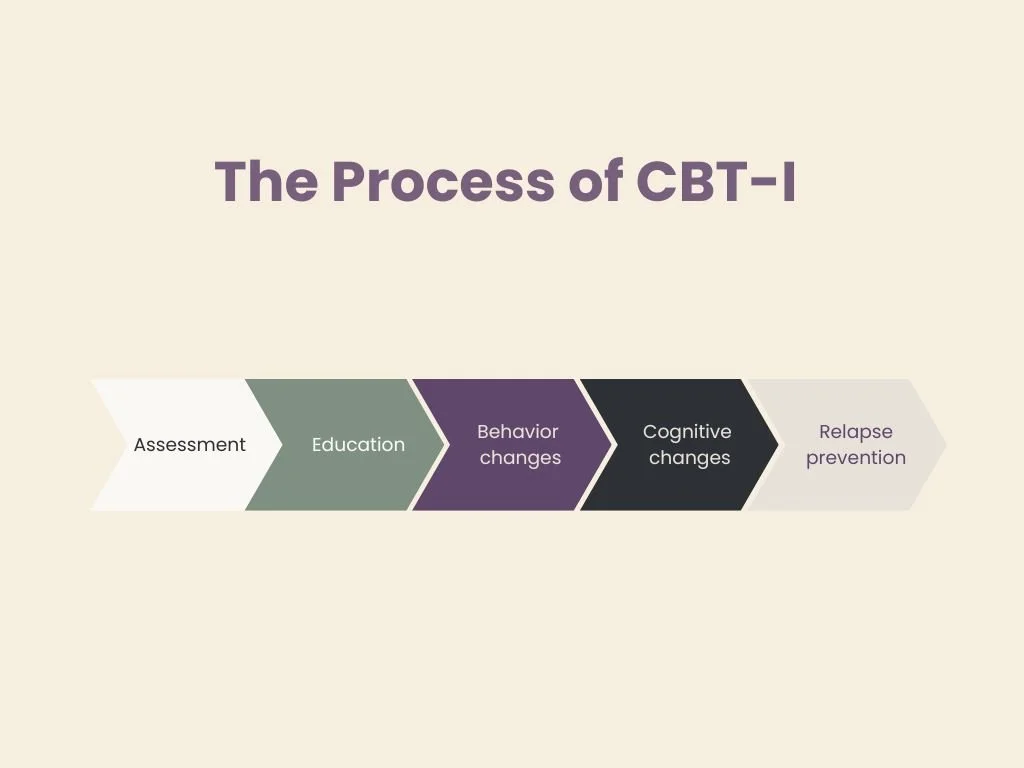
What to expect from CBT-I treatment
We'll begin with a careful assessment.
Before deciding on treatment, I want to make sure we're treating insomnia—and not another sleep disorder that looks similar.
Once we have a sense of what's happening, we'll build a treatment plan together.
Throughout treatment, I'll explain the reasoning behind every recommendation.
If I suggest spending less time in bed, I’ll explain why.
If we're changing your wake time, you'll know what we're trying to accomplish.
My goal is not just to give you a list of things to do. It's for you to gain enough knowledge about your sleep that what we're doing makes sense.
Before we decide how to treat your insomnia, we have to know what's keeping it going.
We have to understand it before we can change it.
Is CBT-I Right for You?
CBT-I is often a good fit if:
you dread bedtime because you expect another bad night
you've been struggling for months or years
you've tried sleep hygiene without much success
you're looking for a treatment that addresses the cause of chronic insomnia rather than temporarily masking it
you want to understand how your sleep works instead of simply being told what to do
Frequently Asked Questions About Insomnia Treatment in Austin
-
Cognitive Behavioral Therapy for Insomnia (CBT-I) is an evidence-based treatment designed specifically for chronic insomnia. Rather than focusing only on sleep hygiene or relaxation, CBT-I addresses the thoughts, behaviors, and patterns that can keep insomnia going over time.
-
Sleep hygiene can be helpful for supporting healthy sleep, but it is not considered a treatment for chronic insomnia. Many people with insomnia have already tried improving their sleep habits without significant improvement. CBT-I goes beyond sleep hygiene by targeting the factors that maintain insomnia.
-
Many people who seek CBT-I have already tried supplements, medications, meditation, relaxation techniques, and sleep hygiene recommendations. Insomnia often persists because the factors maintaining it have not been fully addressed. Treatment begins with understanding what's contributing to your sleep difficulties and developing a plan tailored to your situation.
-
Not necessarily. Some people choose to continue using sleep medication, while others are interested in reducing or discontinuing it. Any medication changes should be discussed with the prescribing provider. CBT-I can be effective whether or not someone is taking sleep medication.
-
CBT-I is typically a short-term treatment. The exact length depends on your sleep history, goals, and individual circumstances, but many people begin noticing changes within the first several weeks of treatment.
-
Sleep problems often begin during periods of stress, illness, pain, anxiety, or other life challenges. However, insomnia can sometimes continue long after the original trigger has improved. That's one reason insomnia often benefits from targeted treatment rather than assuming it will resolve on its own.
-
Yes. CBT-I has been shown to help many people with long-standing insomnia. In fact, some of the people who benefit most are those who have struggled with sleep difficulties for years and feel like they've already tried everything.
-
100%. Insomnia is a learned behavior that has become a habit. Habits are changeable through changing behaviors.
Let's Untangle Your Sleep
Living with insomnia is exhausting.
Not just because you're tired. Because you're not getting a good return on investment for all the effort you're putting into trying to sleep.
The encouraging part is that none of this means you've forgotten how to sleep.
Your brain is doing exactly what human brains do. It's learned a pattern. And learned patterns can change.
The first step isn't trying harder. It's recognizing what's happening.